
Dentofacial orthopedics for problems of skeletal aetiology
Dentofacial orthopedics are used to correct any type of jaw problems of skeletal aetiology.
As children and adolescents have the potential to grow, this provides a unique opportunity for the treating Specialist Orthodontist to intervene and redirect jaw growth into a more favorable pathway, up to an extent.
Patients and parents often wonder and ask us the duration of dentofacial orthopedic treatment. It is the same general body growth principles that also apply in facial and jawbone growth. A good example is that just as a growing child cannot go to sleep and wake up the next day 10cm taller, so it is with the face and the jaws. Therefore, dentofacial orthopedics usually last around 9-12 months to provide the tissues with the necessary time to respond, remodel and grow.
The severity of the problem and the anatomic limitations imposed by the perioral tissues and face esthetics are the most important determinants that define the boundaries within which we can act for successful, healthy, esthetically pleasing, and stable long-term results.
Constricted maxilla (upper jaw)
When the transversal relationship between the upper and the lower jaw is normal, the upper teeth “hug” the lower ones meaning they are forming a wider arch around the lower teeth.
A narrow maxilla is usually accompanied by a narrow and high-arch palate and a posterior cross-bite, which can be either unilateral or bilateral.
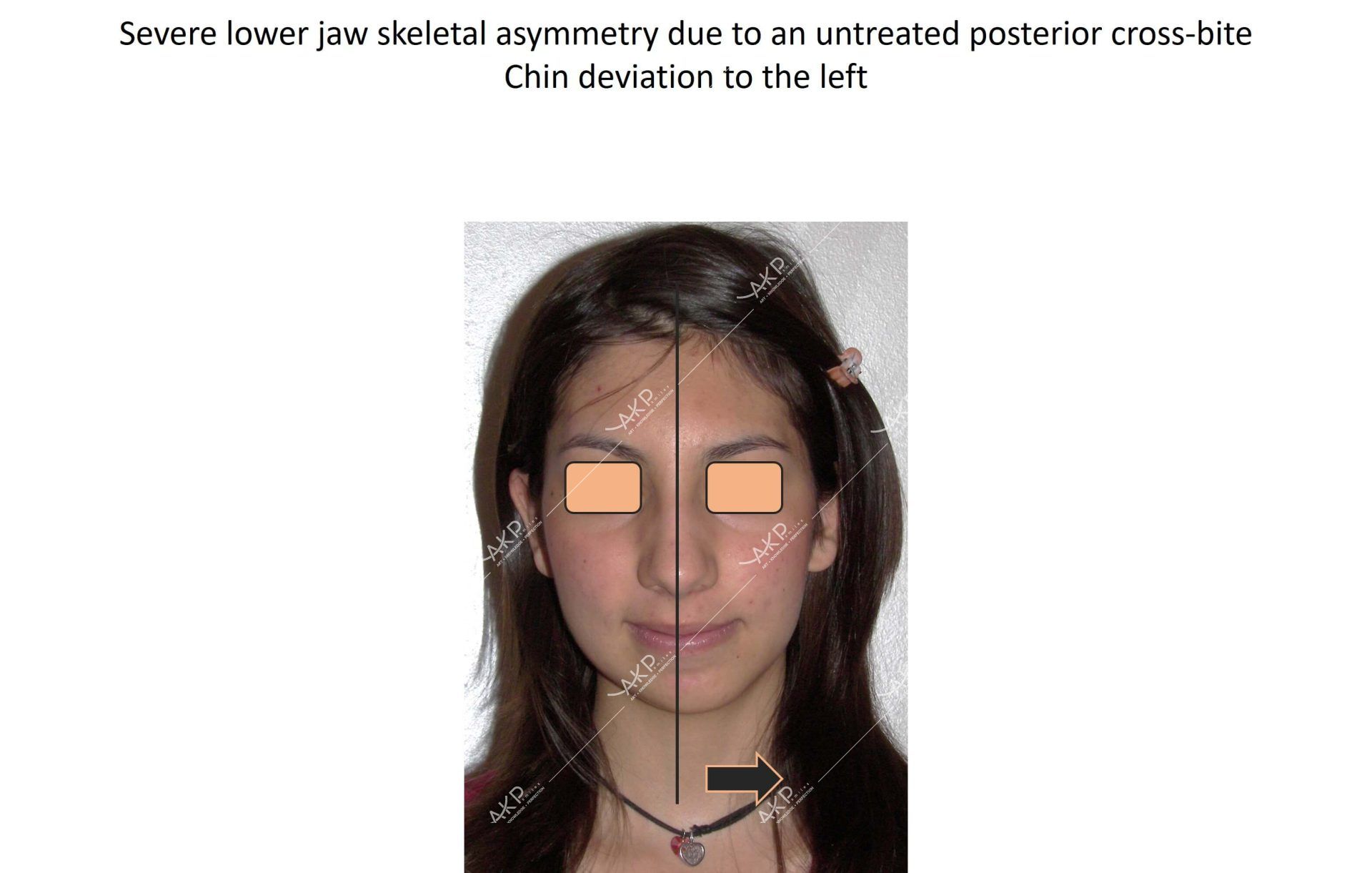
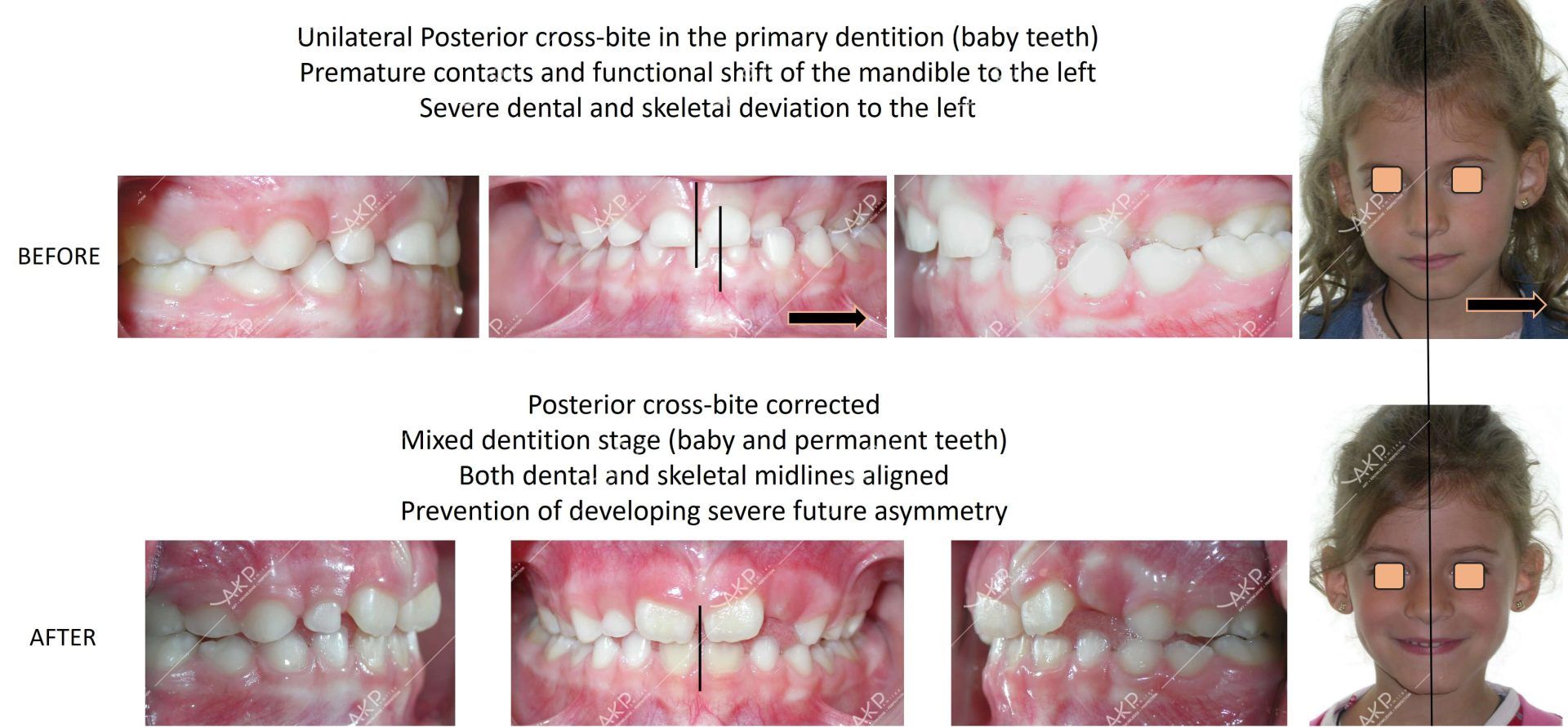
Despite the greater amount of transversal discrepancy between the jaws in cases with bilateral posterior cross-bite, it is the unilateral posterior cross-bite that if left untreated can create more severe side-effects such as skeletal asymmetries. As the lower jaw cannot find a comfortable position to bite, it shifts on the one side (either right or left) and establishes a locked asymmetric position in occlusion, a condition that leads to asymmetric skeletal growth. If the situation is diagnosed and treated in a timely manner with maxillary expansion, proper alignment of the jaws is achieved, and their growth continues normally.
There are several designs of maxillary expanders used to treat a narrow maxilla and the selection depends on problem severity and the skeletal maturation stage of your child. By applying specific criteria, we can identify this stage and design the expander accordingly. In this way, we achieve safe and successful maxillary expansion with transversal coordination between the upper and the lower jaw, both of which subsequently lead to better function and ameliorate the smile esthetics of our patients.
Retrognathic mandible (lower jaw)
The ideal relationship between the upper and the lower teeth and jaws is that the upper ones are around 2mm in front of the lower ones.
Patients proceed very often for orthodontic examination with the chief complaint that the upper teeth are sticking out; however, in most of the cases the main problem is due to deficient lower jaw growth (mandibular retrognathism), which sometimes is combined with excessive upper jaw growth. In children and adolescents, dentofacial orthopedics are directed towards controlling the aetiology for resolving this type of skeletal discrepancy.
The jaw correctors deliver dentofacial orthopedic forces to achieve ideal sagittal coordination of teeth and jaws. These appliances can be either removable or fixed.
After or simultaneous to this dentofacial orthopedic phase, orthodontic treatment is completed either with conventional braces/brackets or aligners.
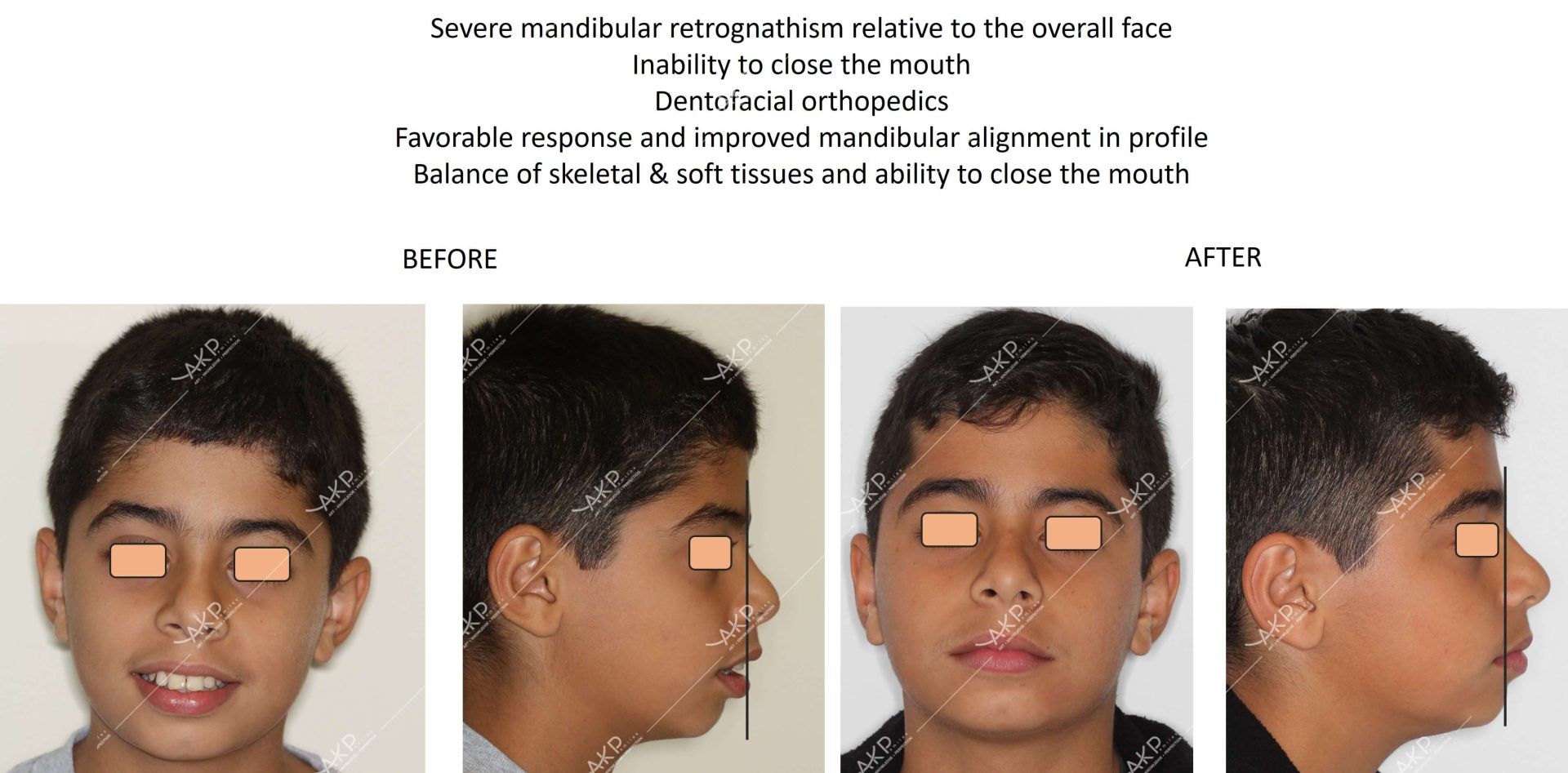

Treatment response to dentofacial orthopedics or future relapse varies and relies on the severity of the problem, patient’s compliance, each patient’s growth potential and the biologic/genetic background of bones and neuromuscular tissues.
Retrognathic maxilla (upper jaw)
The ideal relationship between the upper and the lower teeth and jaws is that the upper ones are around 2mm in front of the lower ones.
In cases that this relationship goes in the opposite direction, we see the lower teeth sticking in front of the upper ones. This situation is characterized, most of the times, by a discrepancy in the amount and direction of growth between the jaws. This malocclusion is heavily linked to genetic factors and either one or both parents have a similar problem, or it can even go back to previous generations.
In 60% of the cases, the problem arises from a small upper jaw (retrognathic maxilla). The rest of the cases have either a big lower jaw (mandibular prognathism) or a combination of small upper and big lower jaws.
Unfortunately, restriction of the lower jaw growth cannot be controlled with any kind of orthodontic or orthopedic appliances while these patients also grow for longer periods of time relative to the general population. While growth is completed in adolescence for most of the general population, these patients continue to grow even after the age of 20 years. Another limiting factor in excessive mandibular growers is that with today’s available technology and methods, no one can predict how much more and for how long the lower jaw will continue to grow for each individual patient.
There is also great news! We have a plethora of methods that facilitate maxillary (upper jaw) forward protraction (movement). As mentioned, more than half of the cases with such malocclusions have a retrognathic maxilla so dentofacial orthopedics are focusing on this direction.
Temporary anchorage devices (TADs) have enormously expanded the boundaries and potentials for enhanced maxillary protraction, limiting the need for future orthognathic surgery, and with most cases being successfully treated with excellent dental and harmonious skeletal and facial results that remain stable over time.


Treatment response to dentofacial orthopedics or future relapse varies and relies on the severity of the problem, patient’s compliance, each patient’s growth potential and the biologic/genetic background of bones and neuromuscular tissues.
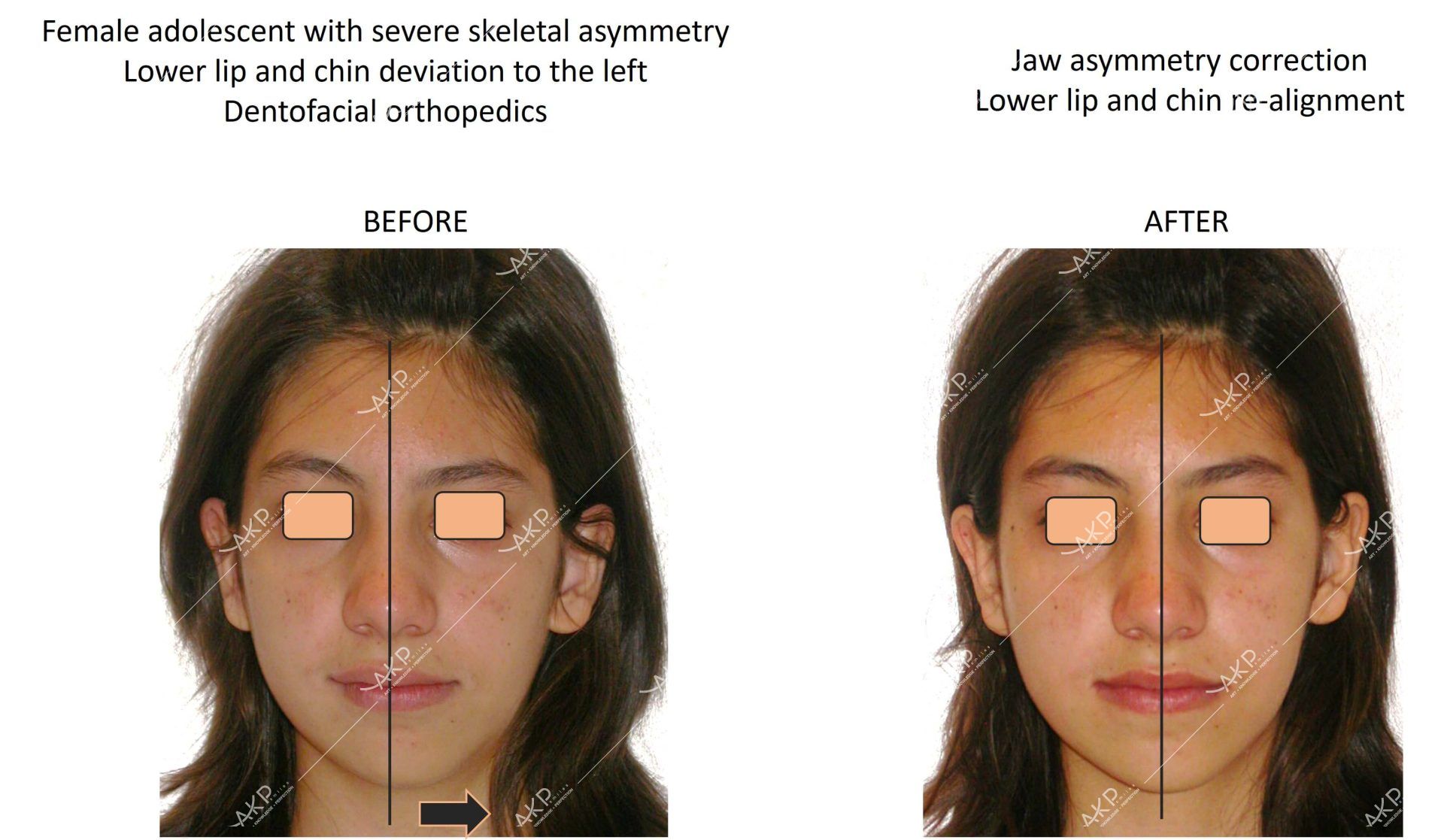
Asymmetries
Asymmetries are defined as any imbalance or discrepancy between the right and the left side of the face.
All faces have some type of minor asymmetry, which is considered normal and esthetically pleasing, even from the ancient years as depicted in ancient Greek sculpture and art. It is extreme deviations of well above 2mm that can be obvious and easily recognizable not only by the orthodontists but also by the patients.
The aetiology is multifactorial and can be of:
- developmental embryonic origin
- condylar growth deviations such as
- hyper/hypoplasia
- habits
- face trauma with condylar fractures and ankylosis
- lower jaw deviations due to premature contacts and mandibular shifts at closure
- soft tissue imbalances (face muscle hypertrophy or atrophy)
- neuromuscular degenerative pathologic conditions.
Orthodontic and dentofacial orthopedic diagnosis and treatment approaches in growing patients with asymmetries aim to accurately specify and eliminate the aetiology to resolve the problem.
Asymmetries develop in all three planes of space (transversal, sagittal and vertical) and can involve bone, teeth, and soft tissues. As a result, in most cases, specific diagnostic procedures are required in order to spot the direction and magnitude of the problem so as to construct a treatment plan that can achieve excellent face esthetics and function.
In rare cases, and especially in cases with suspected unilateral excessive condylar growth, we may prescribe additional medical examinations, in consultation with medical specialists, to decide the type and timing of orthodontic treatment.
Treatment response of asymmetric patients to dentofacial orthopedics or future relapse varies and relies on the severity of the problem, patient’s compliance, each patient’s growth potential and the biologic/genetic background of bones and neuromuscular tissues.
Vertical problems
Vertical problems of skeletal origin are expressed as deficient or excessive vertical growth of the jaws and are closely linked to the composition of face muscles, meaning that they heavily depend on both genetic and environmental/functional parameters of the neuromuscular system. These can be accompanied by dental problems such as deficient or over-eruption of front teeth and/or back teeth expressed as anterior open bite or deep bite.


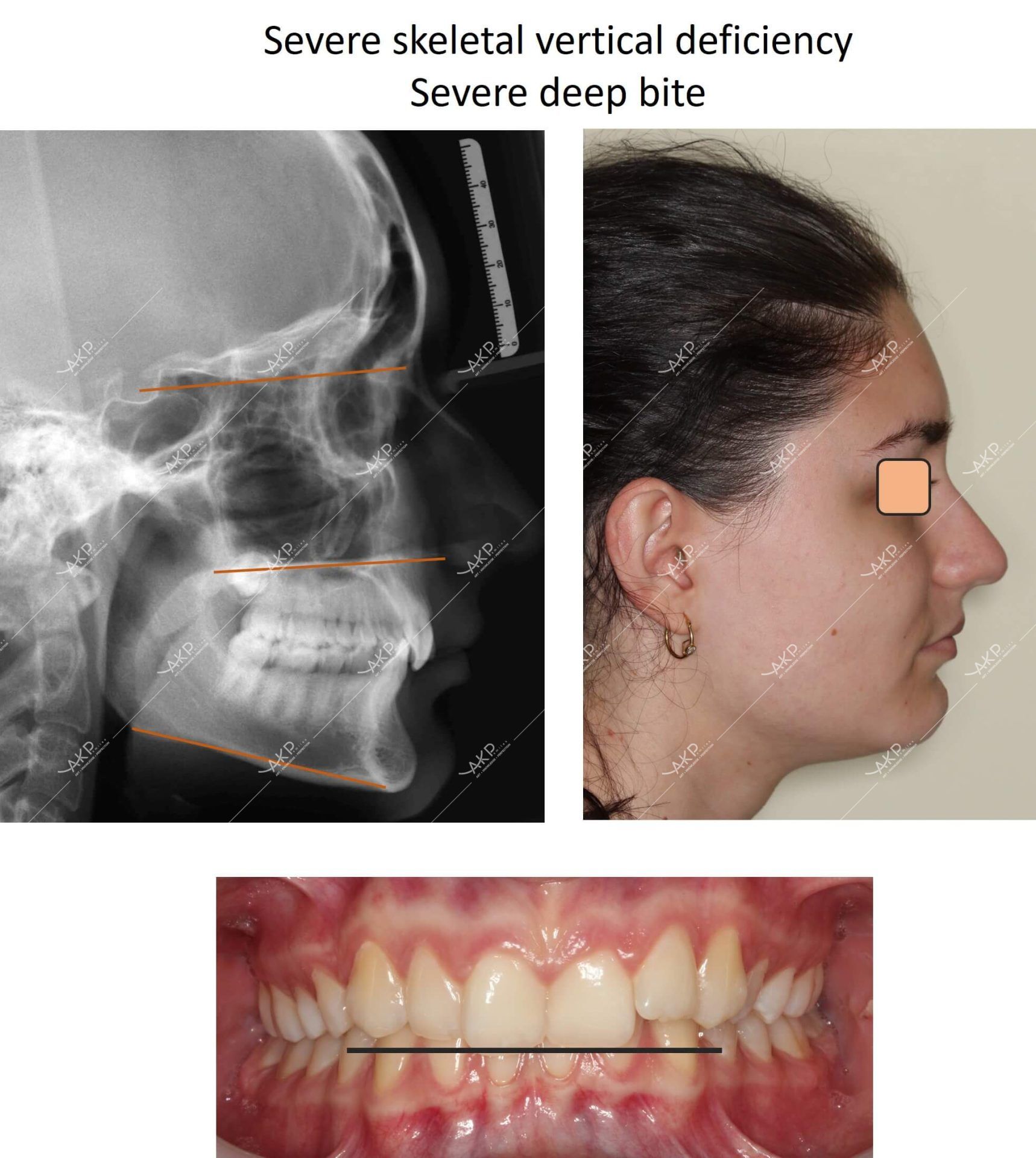
Problems in the vertical dimension are met either as sole problems or in combination with transversal and/or sagittal problems. They are always accounted for when constructing a complete three-dimensional orthodontic treatment planning that aims to achieve ideal dental relationships and occlusion, pleasing aesthetics and harmoniously balanced facial proportions for our patients.